The Science of Healthy Fats

The world is waking up to the reality that sugar and refined carbohydrates are more to blame for the diseases of western civilization than salt or fats. Still, there remains confusion about the health implications of consuming fat. What does modern research have to say about the effects of saturated fat, omega-3s/6s/9s, and short/medium/long-chain triglycerides? What are nutritionists referring to when they use the term “healthy fats”, and what exactly makes fat healthy versus unhealthy?
My goal in this article is to introduce the biochemistry of triglycerides and fatty acids in order to help you understand why the fat in fish, avocados, and olive oil, for example, tend to be healthier for us than the fats in donuts, french fries, and pizza.
After a quick summary, we’ll first examine the various types of fat molecules and their routes from our mouths to our bloodstream. Then we’ll discuss cholesterol’s relationship with fat and look at their combined impact on notable disease symptoms. Finally, we’ll conclude with an examination of the metabolic fates of consumed fats and walk through a practical guide for healthy cooking (and eating) with oils.
Quick Summary
Remember to discuss all this with your doctor carefully before changing your diet. I’ll explain all these concepts, terms, and research in much greater detail below.
- It’s healthy for most people to aim for a 2:1:1 balance between omega-6s, 3s, and 9s, respectively.
- Saturated fat isn’t as bad as we’ve been led to think.
- Swapping carbs with saturated fat has been shown to improve important health markers.
- Swapping saturated fats with omega 3s and 9s is still generally good advice, but it’s less important than you might think.
- Avoid trans-fats.
- Slowly ramp up eating more medium-chain triglycerides (i.e. MCTs, which are fantastic for gut health, energy & mood levels, and mental clarity)
- Eating eggs and meat from grass-fed vs. corn/soy-fed animals actually matters. There are more omega-3s in grass-fed animals.
- Avoid oils high in omega-6s (notably corn, sunflower, soybean, and cottonseed oils).
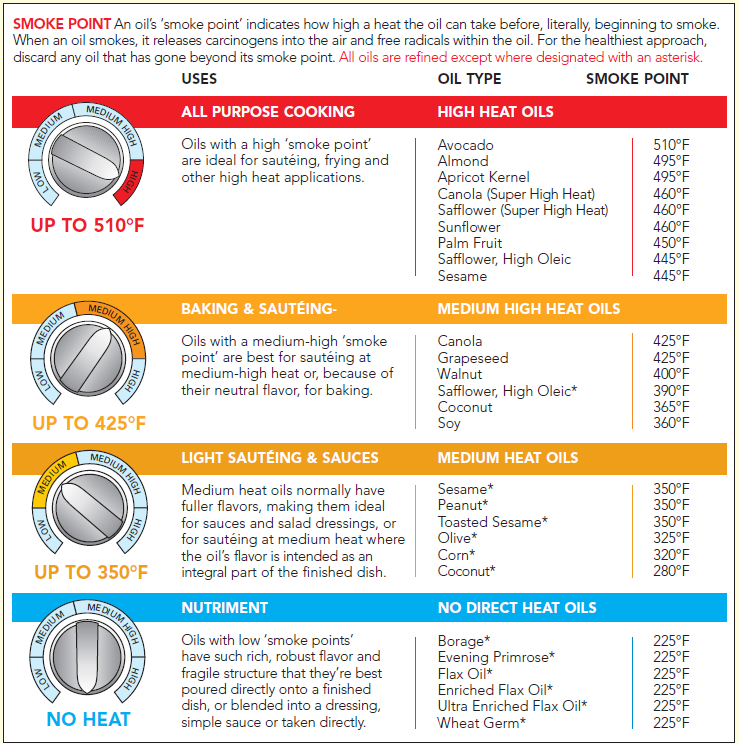
- Heating up oils past their “smoke point” can turn healthy fats into extremely unhealthy fats.
- Eat more fish, olives, and avocados (including their oils).
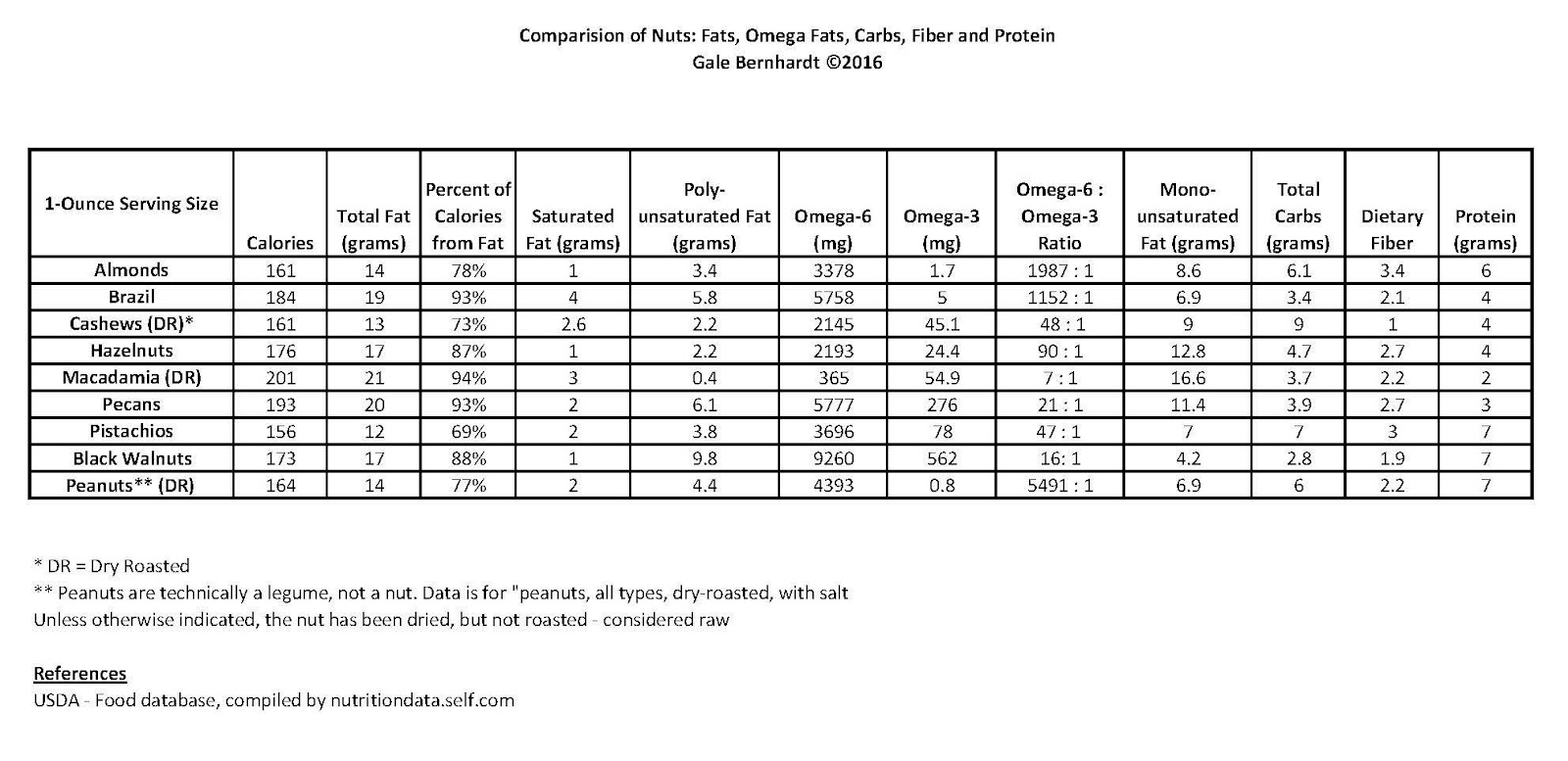
- Go easy on nuts because of their omega-6 content. That being said, a notable low-omega-6 option is macadamias nuts. Runner ups include cashews and hazelnuts, although these have more carbs than other nuts, making it hard to win here (I have a huge list of options below).
- Read my previous articles on the science of salt and electrolytes and ketogenic dieting as important complements to this article, especially if you are experimenting with low-carb, high-fat diets.
What are fat molecules?
The terms “oil”, “fat”, and “lipid” are often used interchangeably. Technically, a fat molecule is sub-category of lipids called a triglyceride, i.e. three chains of fatty acids attached to glycerol backbone:
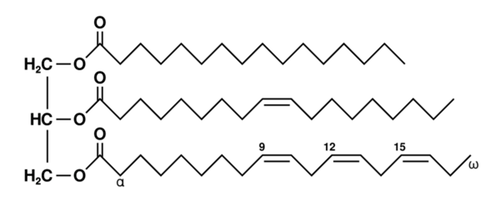
Fatty acid chains come in all kinds of shapes and sizes. In the image above, we’re looking from top to bottom at a saturated, monounsaturated, and polyunsaturated fatty acid chain, respectively.
- Saturated means all the carbons in the chain have maximized the number of hydrogen atoms that can be bonded to it. These types of fats tend to be solid at room temperature because they can pack together tightly.
- Unsaturated means that one (monounsaturated) or many (polyunsaturated) double bonds exist along the chain, which makes the chain “branch” in different directions and not pack as tightly together. These types of fats tend to be liquids at room temperature, which are commonly called oils.
In most naturally occurring unsaturated chains, the configuration of the chains at either side of the double bonds is in the cis form (i.e. same side), but some processed fats — which we’ll talk more about below — can also contain trans configurations, where the chain extends on the opposite side of the bond like this:
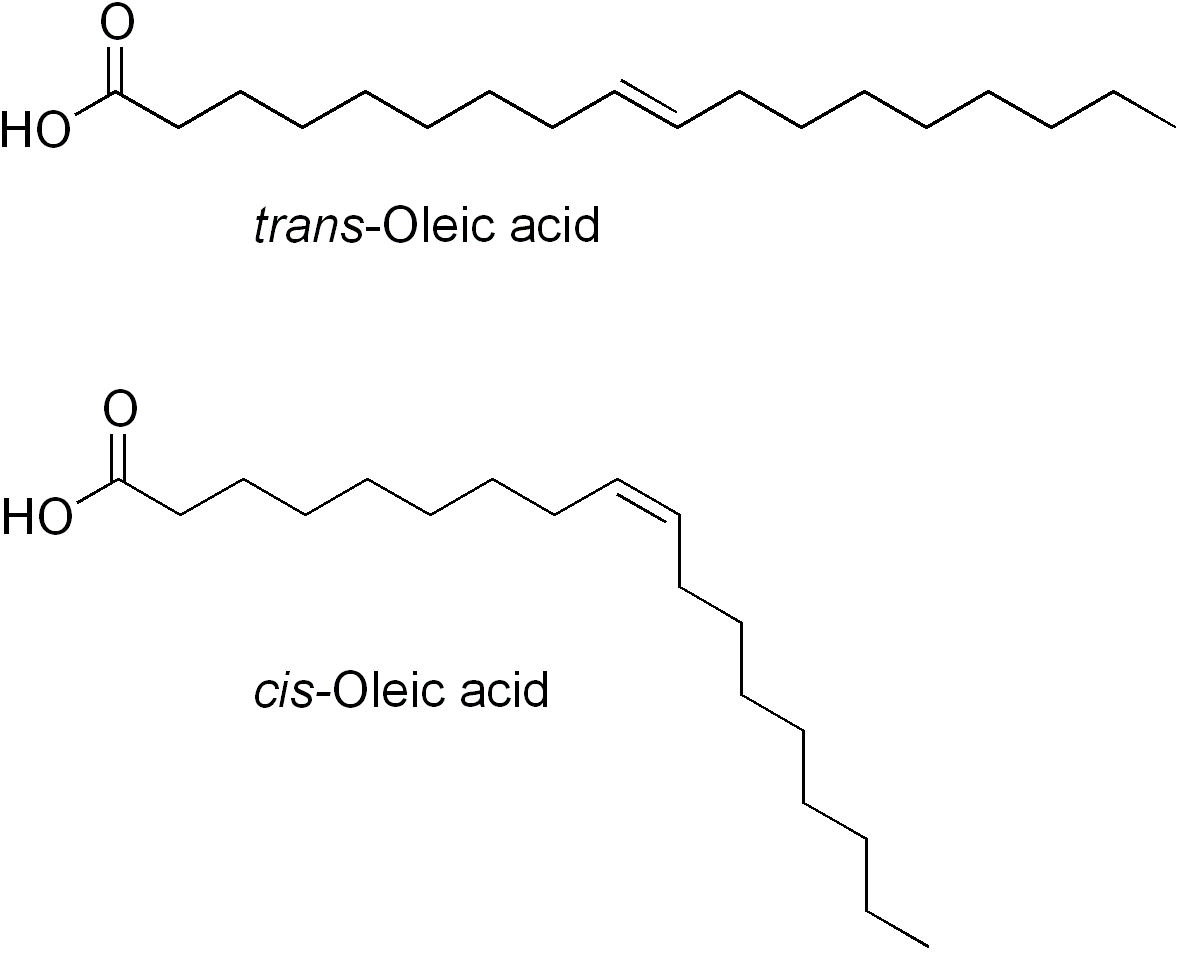
cis-oleic acid is the main type of fatty acid found in olive oil, for example
Why and how are trans-fats manufactured?
Trans-fats are relatively cheap to make and help give food a desirable shelf-life, texture, and taste. Fast food restaurants will commonly use trans-fats in their friers, for example, since trans-fats remain reasonably stable after multiple uses.
The most common food ingredient that contains trans-fats is partially hydrogenated vegetable oil, which can be soybean, corn, safflower, canola, cottonseed, and/or peanut oil infused with hydrogen to saturate some, but not all, of the double bonds along the chain. This process will produce trans-fats in a 2:1 ratio to cis-fats because of the favorable energy state of a trans-fat.
What are omega-3, omega-6, and omega-9 fats?
Unsaturated fatty acid chains where the first double bond starts at the 3rd, 6th, and 9th carbon from the (omega, aka methyl) end are omega-3s, 6s, and 9s, respectively:
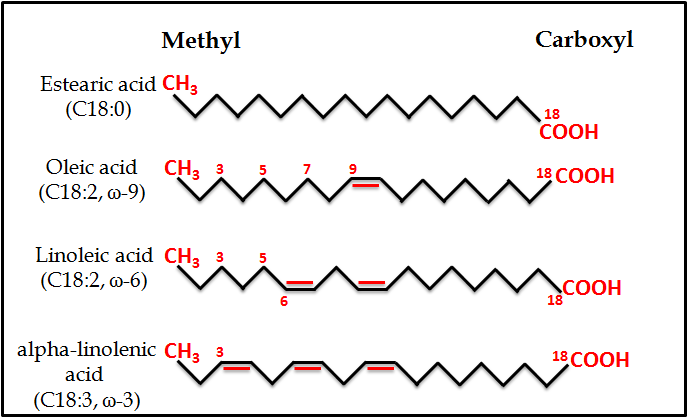
1 saturated and 3 unsaturated fats, showcasing the common omega 3, 6, and 9 unsaturated varieties (ref).
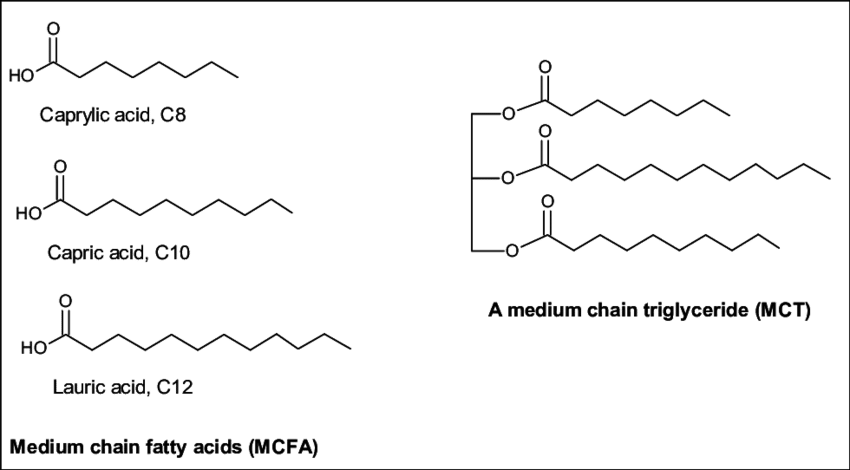
What are medium-chain triglycerides (MCTs)?
If you’ve heard of the bulletproof coffee phenomenon, then you’ve probably also heard of MCT oil, which is often derived from coconut oil and consists of fatty acid chains that have between 6 and 12 carbons:
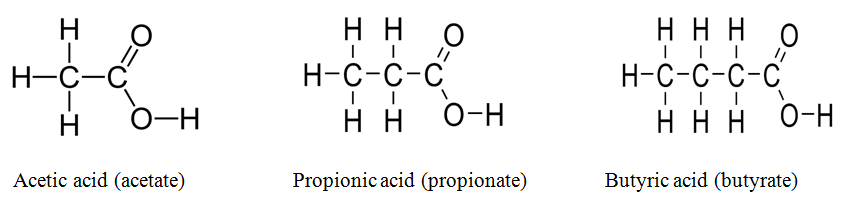
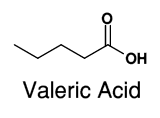
And yes, there are also short-chain fatty acids (5 or less carbons):
And long-chain fatty acids (LCFA), where those with more than 21 carbons are called very long chain fatty acids (VLCFA):
http://www.benbest.com/health/essfat.html
How are fats digested after we consume them?
Now that we’ve looked at all the varieties of fats that exist (i.e. from chain length, bond conformations, and hydrogen saturation levels), let’s address what makes them “healthy” or not.
To start, it’s important to note that fats we consume are mixed with bile sales, cholesterol, and lecithin to form emulsified fat droplets that are “cut” with lipase enzymes and packed into “mixed micelles”:
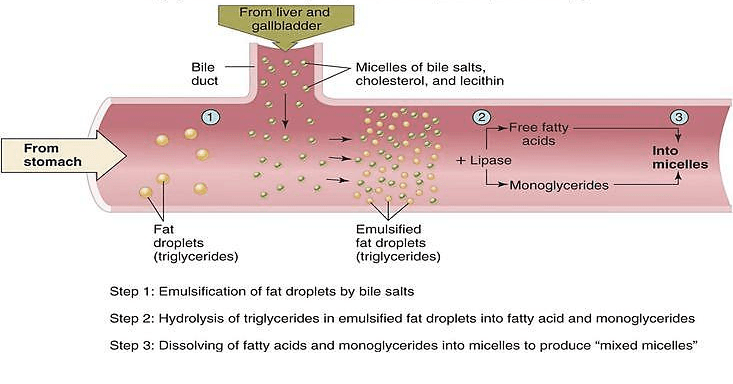
These mixed micelles then passively diffuse into cells lining the intestinal wall:
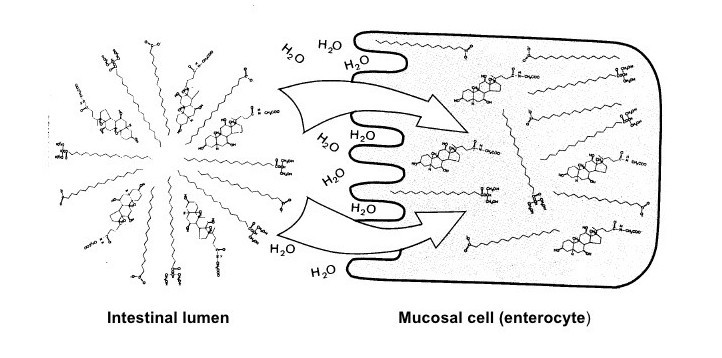
From here, long-chain fatty acids, cholesterol, and fat-soluble vitamins are processed into chylomicrons that enter the lymphatic system (i.e. not the blood quite yet):
Importantly, short- and medium-chain fatty acids skip the chylomicrons and enter the portal vein directly to be metabolized quickly for energy by the liver, where as the chylomicrons enter lacteal lymph vessels around the intestines, collect from lacteal vessels into the thoracic duct, and are eventually emptied into the blood stream via the subclavian vein.
What happens to the chylomicrons once they are dumped into the bloodstream?
The “nascent” chylomicrons that first enter the blood stream quickly mature into full chylomicrons and then circulate around the body to deliver triglycerides to cells around the body (notably fat and muscle cells). They then get processed by the liver once most of the triglycerides are gone:
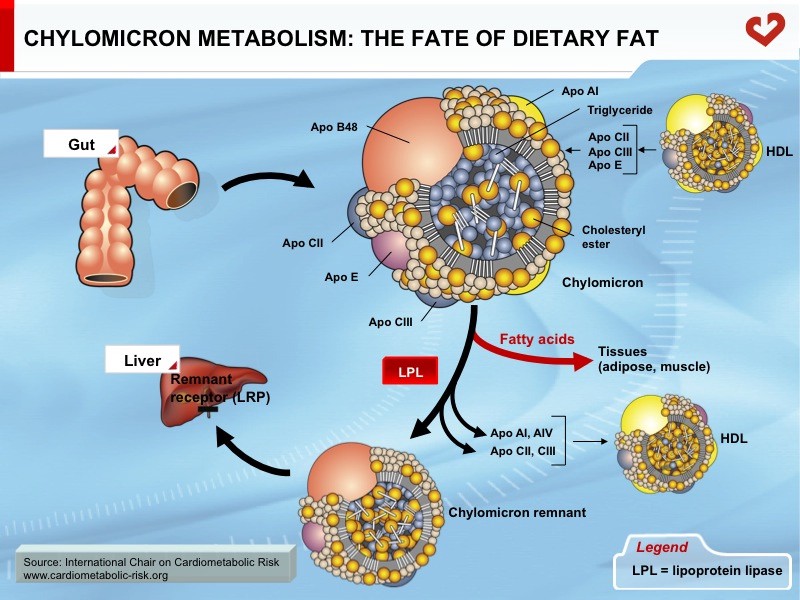
Interestingly, because unsaturated fats can’t be packaged as tightly as saturated fats, unsaturated fats tend to be more easily moved into cells and burned for energy.
How are cholesterol, HDL, and LDL involved?
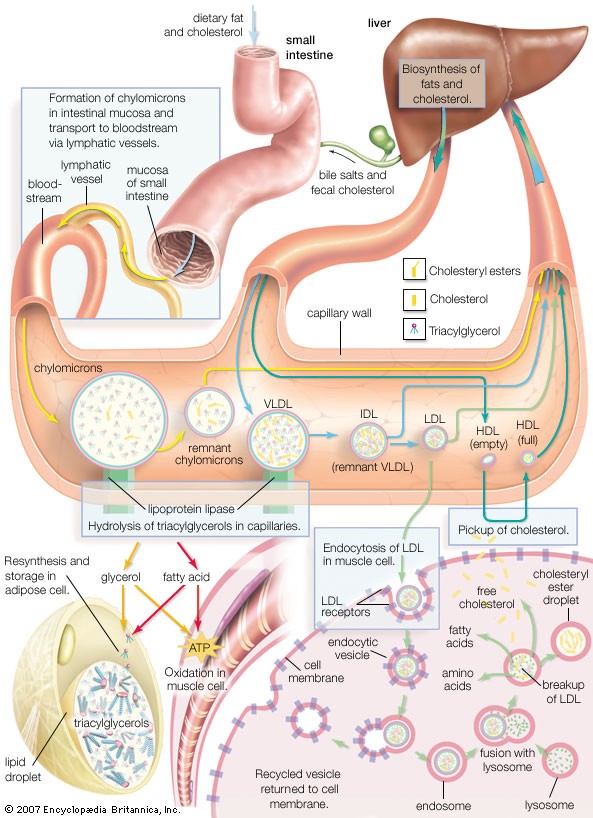
As we discussed above, cholesterol is adsorbed along with vitamins and fatty acids into the cells lining the intestines and transported in chylomicrons around the lymph and blood. Since blood is water-based and fats aren’t soluble in water, spherical lipoproteins (such as chylomicrons) are needed to transport many lipids (such as cholesterol and triglycerides) around the body.
Importantly, the size and density of the lipoproteins vary. The various states commonly found in our bodies have been given names (HDL stands for “high-density lipoprotein”, and LDL = “low-density lipoprotein”, IDL = “intermediate density lipoprotein”, VLDL = “very-low density lipoprotein”):
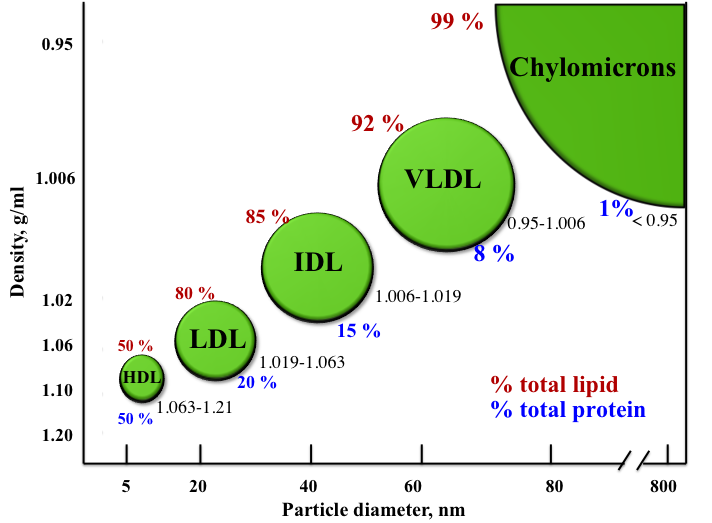
As you might expect, these lipoproteins have different functions in our bodies. While I won’t get too deep into those functions in this article, in general HDL is used to “scavenge” lipids (notably cholesterol) from tissues back to the liver, and VLDL/IDL/LDL/ send lipids from the liver to other tissues.
Here is a quick glance at how they all work together to move fat and cholesterol around the body:
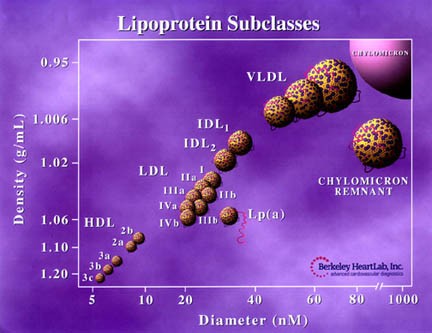
And finally on the topic of lipoproteins, to make matters even more complicated there are a variety of sub-types:
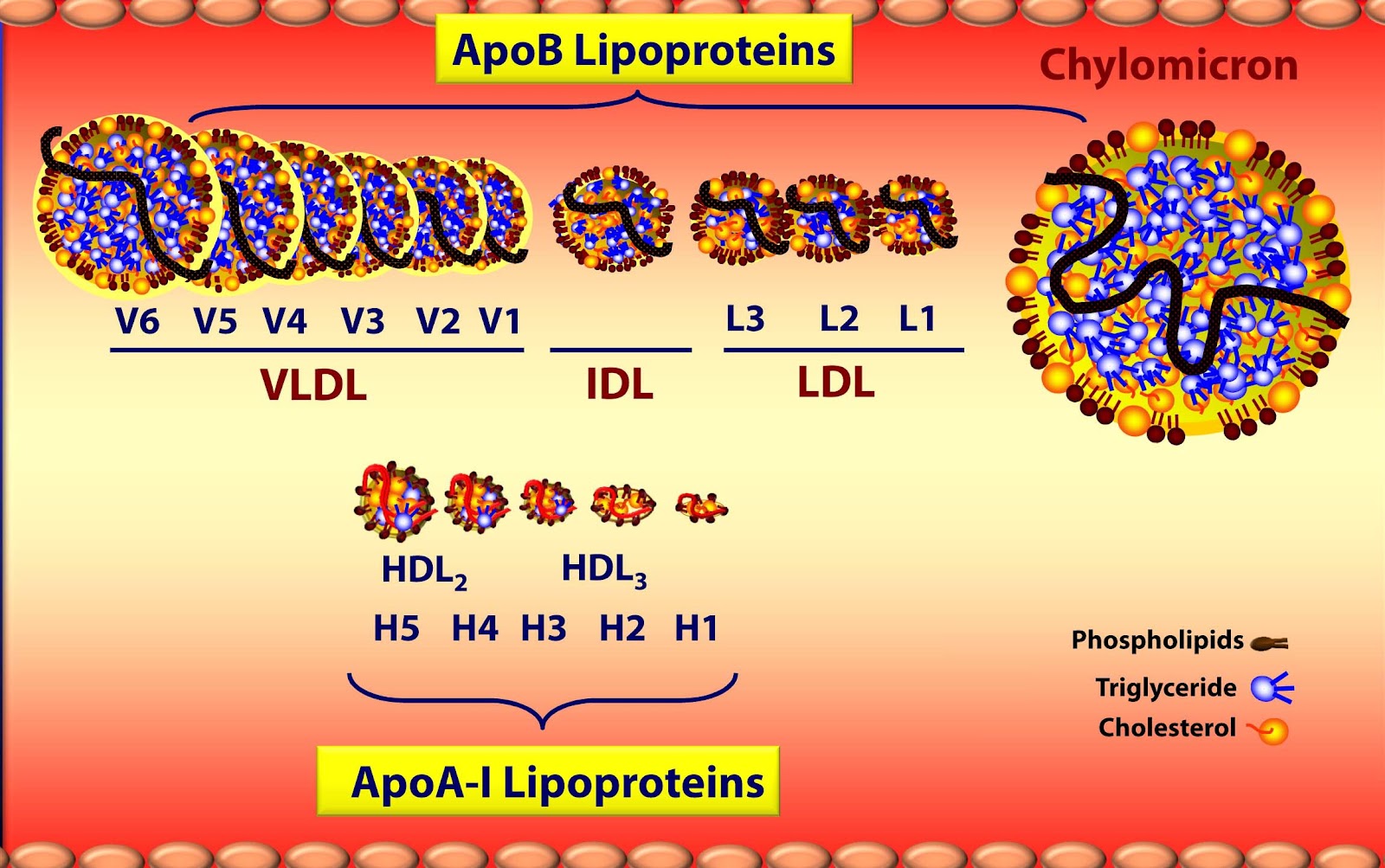
Many of which are divided into even further subclasses:
Each of these subtypes have their own subtle nuances in terms of how they affect our physiology. For example, medical professionals are realizing that the amount of cholesterol in these lipoproteins (e.g. “HDL-C” and “LDL-C”) is less important to cardiovascular disease than the total number of the various sizes of HDL and LDL.
In other words, the number of HDL or LDL in your blood isn’t necessarily correlated with the amount of cholesterol contained in those lipoproteins. If your LDL-C is, say, 130mg/dl, the number and size of those particles matters:
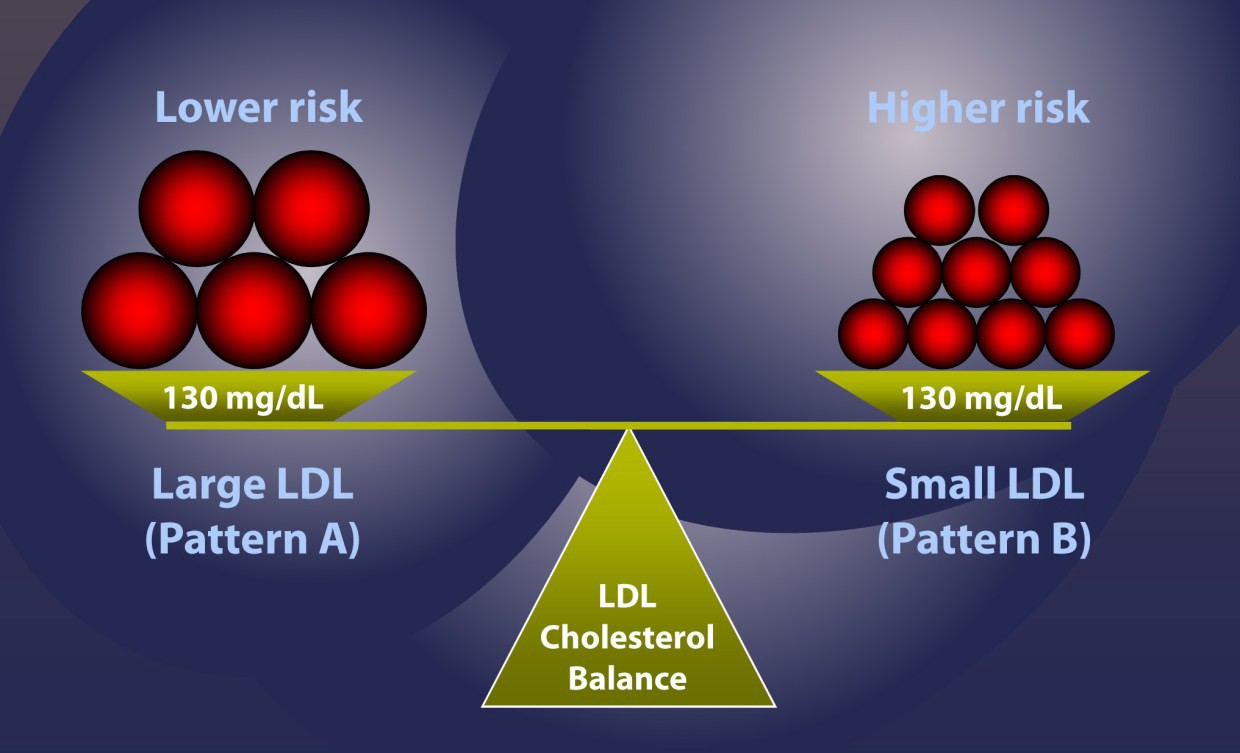
Those smaller LDL particles happen to be the right size and density to lodge themselves in blood vessel walls and cause problems, whereas the the larger and more “fluffy” LDL particles are less of a risk.
How do the various types of consumed fat behave differently in the body?
In addition to the shorter path to the blood stream that medium-chain and short-chain fatty acids take, once in the blood they are able to enter cells — and mitochondria within cells — without the aid of membrane transport proteins. This explains why MCTs provide energy to the body significantly faster than LCTs.
However, Trans-fats consumed in abnormally large amounts (i.e. more than~8% daily energy intake) have a wide host of scary side effects, including:
- Producing abnormally large amount of visceral fat deposits
- Endothelial dysfunction (which precedes atherosclerosis)
- Systemic inflammation
- Reduced LDL particle size
- Higher LDL-C and Lower HDL-C, and thus a higher LDL-C to HDL-C ratio
- Increased serum triglycerides
- Increase insulin resistance (leading to diabetes)
Saturated fats, in and of themselves, are no longer shown to be correlated with an increased risk for cardiovascular disease. They do raise LDL-C for ~25% of the population (i.e. “hyper responders”), but in these cases HDL is also raised, eliminating the potential risk for heart disease based on HDL/LDL ratios.
In addition, consuming saturated fats in place of carbohydrates keeps triglycerides down, and has been shown to decrease the number of LDL particles and therefore removing the harmful “small-dense” LDL kind.
That being said, experts agree that it isn’t necessarily a bad idea to replace saturated fats with unsaturated fats, as doing so has been shown to lower LDL, raise HDL, and lower triglycerides.
Specifically, polyunsaturated fats (omega-3s & omega-6s) are essential nutrients; the body can’t synthesize them so they need to be eaten to maintain optimal health. These types of fat molecules incorporate into nerve coverings and cell membranes, and are critical for muscle movement, blood clotting, and a healthy inflammation response.
Monounsaturated fats (omega-9s) found in olive oil and avocados, for example, activate dopamine, strengthen bones, and increase insulin sensitivity.
Replacing saturated fat with monounsaturated and polyunsaturated fats effects total cholesterol, HDL, LDL, triglycerides, and insulin sensitivity like so:

Do the ratios of consumed omega 3s, 6s, and 9s matter?
Omega-3s (specifically ALA, EPA, and DHA mentioned above) get a lot of deserved attention, but what is not talked about as much is the effects of consuming too much omega-6 compared to omega-3s and omega-9s. Doing so can increase inflammation significantly and lead to arthritis, heart disease, Alzheimer’s, and many types of cancer.
Since our bodies can synthesize omega-9s (i.e. it’s not essential), and most people on western diets consume plenty of meat, eggs, dairy, and vegetable oils (i.e. omega 6s), focusing on replacing omega-6s with as many omega-3s as possible is a smart move. When that’s not possible, then replacing omega-6s with omega 9s is second best. (We’ll discuss below the various types of foods to consume to effectively do this).
Ultimately, aiming for a ratio of 1:2:1 for omega 3s, 6s, and 9s, respectively, is where research currently suggests we aim, although practically as long as people on western diets try to consume less than the ~10–50x more omega 6s than omega 3s & 9s we currently do now, then we’ll likely start seeing some the corresponding health benefits.
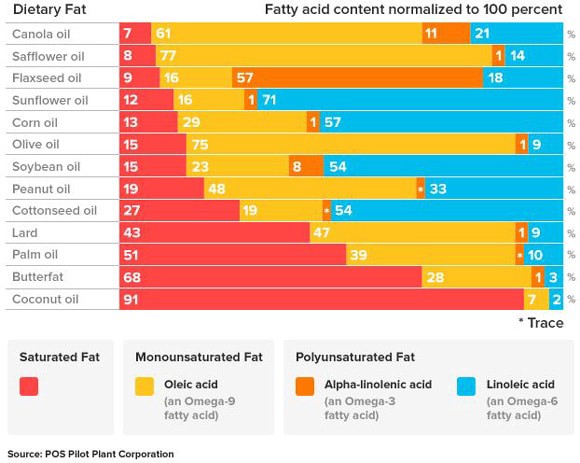
Here’s a helpful chart showing the omega 3/6/9 & saturated fat ratios of common oils:
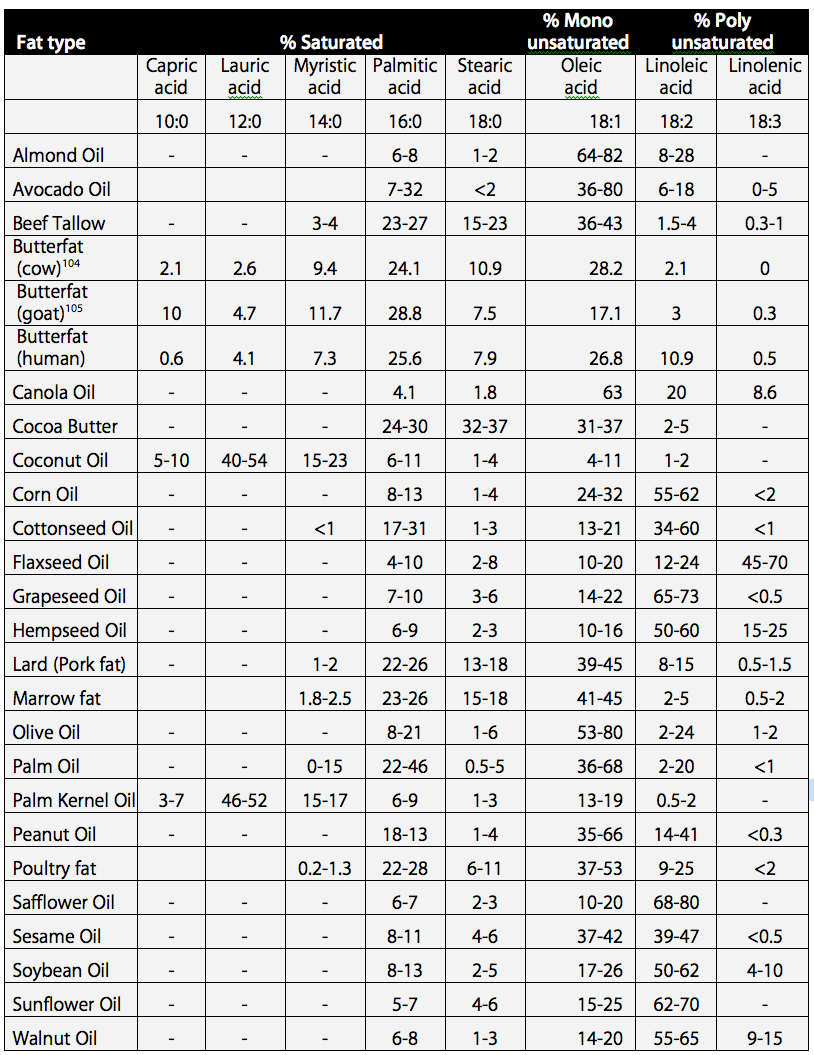
And here is a similar chart from another source that includes other common foods as well:
And to dive more specifically into the length of the saturated chains (capric and lauric acid are MCTs, oleic/linoleic/linolenic acid are omega 9/6/3, respectively. The second row tells you the carbon and bond numbers, as 18:1 means, for example, that there are 18 carbons and 1 double bond)
As you can see from the charts above, assuming you get omega-6s elsewhere (e.g. meat, dairy, and eggs), it is likely a good idea to avoid cottonseed, soybean, corn, and sunflower oil because they are very high in omega-6s.
Furthermore, it’s also a good idea to avoid eating eggs and meat from animals that have been fed these oils (especially corn and soybean oils, which are in most industrial animal feed).
A 2015 study of 32 grass-fed, free-ranged and pastured cows, lambs, pigs and chickens measured the omega 3 vs 6 amounts compared to standard industrial animals and found that omega 3 levels were massively higher:
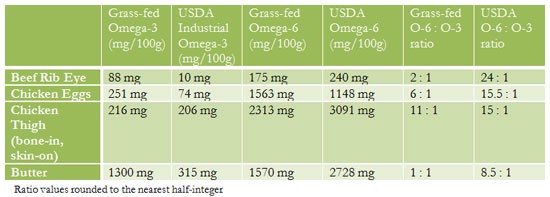
And if you think about it, this makes initiative sense. We’d expect to see higher omega-6 numbers in the fat tissue of animals that are fed omega-6-rich food.
A quick summary of the “good” and “bad”
Up to this point we’ve learned that a “good” blood lipid profile has low LDL (both C & P), high HDL-C, low triglycerides, high HDL/LDL ratio, and a low total-C/HDL ratio.
We’ve also discovered that:
- Omega 3s and 9s are, broadly speaking, “good”
- Trans fats and excess omega-6s are “bad”
- Medium-chain and short-chain MCTs produce quick energy (which is a bonus), and they don’t mess with lipoprotein profiles since they aren’t carried by HDL/LDL/etc...
- Long-chain saturated fats are far superior than carbs, and are likely somewhere between “neutral” and “good” for you depending on your genetics (here is a great article summarizing the current science of saturated fats).
Going deeper: do we know *why* the known positive and negative effects of the various fats occur?
So while it’s common among nutritionists to discuss the symptoms from consuming various types of fats, it’s also important to understand the underlying mechanisms. What do we know about trans-fats and an excess of omega-6s, for example, that causes all the problems discussed above? What is it about omega-3s and saturated fats that — relatively speaking — improve the bad symptoms we’ve been discussing?
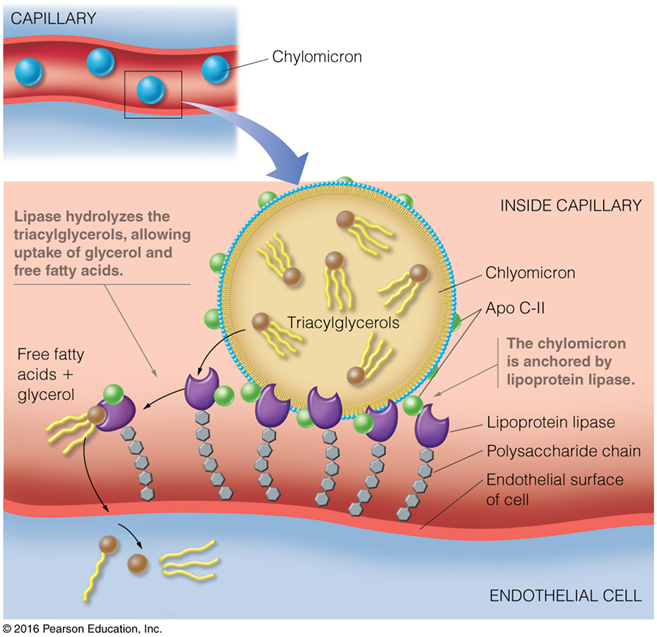
Well, we know that all triglycerides in chylomicrons (from food) and VLDL (from the liver) — independent of what type of fatty acids chains are attached — are transported into cells via a mediated process involving lipoprotein lipase (LPL):
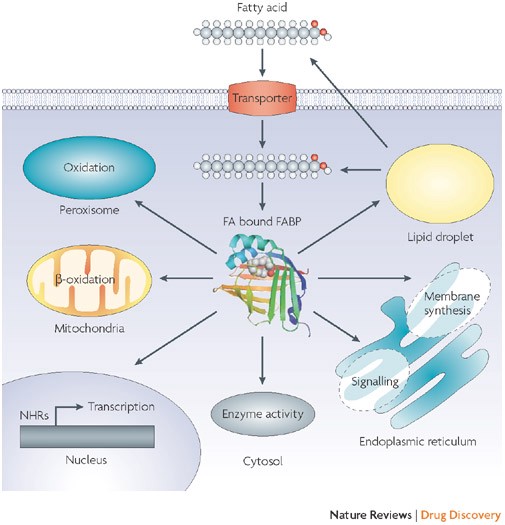
From here, the fatty acids bind to Fatty Acid Binding Proteins (FABPs) and are diverted to a number of roles inside the cell beyond just being oxidized for energy, such as modifying gene expression, enzyme activity, cell signaling, and membrane synthesis:
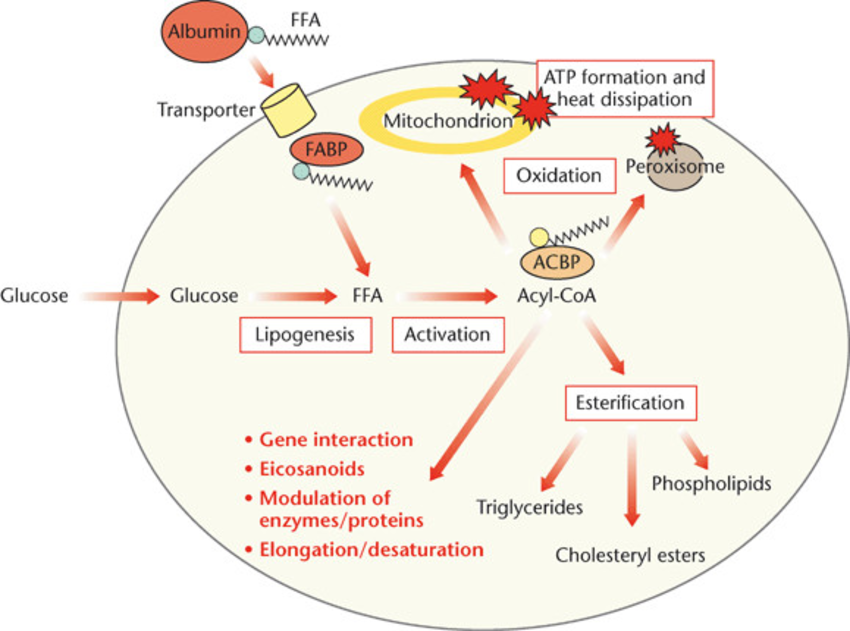
And here is another look at a similar graphic from a slightly different perspective showing the fate of fatty acids in a cell, including those synthesized from excess glucose:
It is undoubtedly a combination of these complex processes that cause trans-fats and an excess of omega-6s to increase inflammation, insulin resistance, LDL (C&P), and serum triglycerides.
For example, a higher amount of omega-6s in our bodies dramatically up-regulates our endocannabinoid system, which increases inflammation, insulin insensitivity, and fat accumulation.
It is also known that trans-fats (TFAs) activate the tumor necrosis factor (TNF) system, which is involved in our bodies’ inflammation response, and may be caused by TFA incorporation into cell membranes:
How might TFA consumption influence inflammation? TFAs are incorporated into endothelial cell membranes, which have numerous cell-specific pathways relating to TNF activation. TFAs may also modulate TNF biology via effects on macrophage membrane phospholipids and signaling pathways, in a manner analogous to mechanisms seen with n−3, n−6, and monounsaturated fatty acids.
Alterations in cell membrane structure by incorporation of consumed TFAs have also been proposed as one of the mechanisms behind the associated increase in insulin resistance.
And as it relates to TFA effects on cholesterol:
a greater proportion of acetyl-CoA was channeled to cholesterol synthesis in the presence of trans fatty acids compared with cis and saturated fatty acids
In other words, consuming TFAs put our bodies in an abnormal state of producing an over-abundance cholesterol.
Furthermore, fatty acids can be converted into a class of signaling molecules called eicosanoids that are involved in a far-reaching set of biological processes:
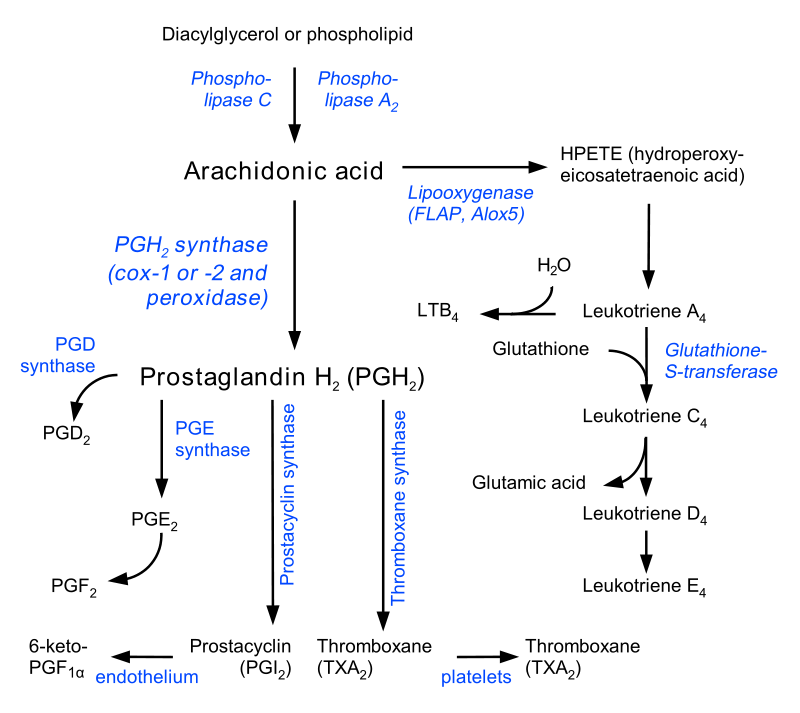
While the nuances of all these processes are beyond the scope of this article, we can now conceptually understand how TFAs and an imbalance of omega 3s, 6s, and 9s can lead to symptoms related to cancer, diabetes, inflammation, auto-immune, and heart diseases.
What foods contain the various fats? What should I eat?
In order to reduce your TFAs and omega 6s, let’s take a quick look at the spectrum of fats found in common food:
Saturated fats
- Medium-chain fatty acids can be found most abundantly in coconut oil and palm kernel oil. Smaller amounts can also be found butter, cheese, and milk.
- Short-chain fatty acids mainly come from bacteria in our digestive system, which can be up-regulated by consuming fiber-rich foods such as fruits, vegetables, and legumes. There are also some short-chain fatty acids (notably butyrate) in dairy products, especially butter.
- Long-chain, saturated fatty acids can be found mainly in animal-derived food (lard, bacon, dairy, beef, eggs, etc…)
Unsaturated fats (monounsaturated and polyunsaturated)
- Monounsaturated fats (especially omega-9s) are found in highest amounts in olive oil, avocado oil, canola oil, safflower oil, macadamia oils, and a variety of other nuts and oils.
- Of the polyunsaturated fats, omega-6s are found in common industrial oils (sunflower, soybean, corn, and cottonseed), as well as in meat and eggs from animals that are fed these oils. Most nuts have a fair amount of omega-6s as well (note the monounsaturated fat is the omega-9)
- Omega-3s are notably from fish and marine animals, but can also be found in meat and eggs from grass-fed animals, as well as in some nuts (per the charts above).
What oils are healthiest (and safest) for cooking?
In general, picking the the high-omega-9 oils (olive, avocado, safflower, canola, etc…) out of the following list to avoid the “smoke point” at the temperatures you’ll be cooking at is the safest and healthiest route:
Additional notes and further reading
While we just scratched the surface of the science behind fats in this article, hopefully you now have a better understanding of how trans fats and an excess of omega-6s can impact cell membrane fluidity, signaling molecules, and other biological processes to create negative downstream effects (inflammation, obesity, cardiovascular disease, etc…).
In addition to the research linked above, to dive even further into inflammation responses that various fats have on the body, follow the rabbit trails not only of TNF-alpha described above, but pay close attention to interleukin 6 (IL-6) and C-reactive protein (CRP), which have their own roles in systemic inflammation and are often correlated with TNF-alpha activity.
Specifically, I’d recommend an article from 2012 in the Journal of Nutrition and Metabolism entitled Health Implications of High Dietary Omega-6 Polyunsaturated Fatty Acids. In fact, I’ll leave you here for now with its abstract, which summarizes much of the science we’ve discussed above:
Omega-6 (n-6) polyunsaturated fatty acids (PUFA) (e.g., arachidonic acid (AA)) and omega-3 (n-3) PUFA (e.g., eicosapentaenoic acid (EPA)) are precursors to potent lipid mediator signalling molecules, termed “eicosanoids,” which have important roles in the regulation of inflammation. In general, eicosanoids derived from n-6 PUFA are proinflammatory while eicosanoids derived from n-3 PUFA are anti-inflammatory. Dietary changes over the past few decades in the intake of n-6 and n-3 PUFA show striking increases in the (n-6) to (n-3) ratio (~15 : 1), which are associated with greater metabolism of the n-6 PUFA compared with n-3 PUFA. Coinciding with this increase in the ratio of (n-6) : (n-3) PUFA are increases in chronic inflammatory diseases such as nonalcoholic fatty liver disease (NAFLD), cardiovascular disease, obesity, inflammatory bowel disease (IBD), rheumatoid arthritis, and Alzheimer’s disease (AD). By increasing the ratio of (n-3) : (n-6) PUFA in the Western diet, reductions may be achieved in the incidence of these chronic inflammatory diseases.
—
Author’s note: thanks in advance for any/all feedback, corrections, and comments to this article. Subscribe to my newsletter and I’ll let you know when I write more about health and fitness topics (FYI: I also write about entrepreneurship, blockchain technology, and other miscellaneous science/tech topics). Special thanks to Tony for help editing this article. And last but not least, remember to comment (which you can also do inline by highlighting something), hit the clap button, and/or share this article with a friend if you’ve found it helpful. Thanks!