The Science Behind Fat Metabolism

Per the usual disclaimer, always consult with your doctor before experimenting with your diet (seriously, go see a doctor, get data from blood tests, etc.). Please feel free to comment below if you’re aware of anything that should be updated; I’d appreciate knowing and I’ll update the content quickly. My goal here is to help a scientifically curious audience know the basic story and where to dive in for further study. If I’m successful, the pros will say “duh”, and everyone else will be better informed about how this all works.
[UPDATE #1: January 18, 2016. Based on a ton a helpful feedback and questions on the content below, I’ve written up a separate article summarizing the science behind ketogenic (low-carb) diets. Check it out. Also, the below content has been updated and is still very much applicable to fat metabolism on various kinds of diets. Thanks, everyone!]
[UPDATE #2 : December 6, 2019. I’ve edited/re-phrased topics below that I’ve learned more about in the last few years, especially in the sections regarding lipoproteins, exercise, and sleep.]
[UPDATE #3 : July 25, 2020. Welcome to the most recent version of this article here on Satchel, a new site I helped build that makes it easy to publish both online and to a newsletter. Subscribe to my newsletter to stay posted as I publish more on health science topics. Thanks!]
tl;dr
The concentration of glucose in your blood is the critical upstream switch that places your body into a “fat-storing” or “fat-burning” state.
The metabolic efficiency of either state — and the time it takes to get into one from the other — depends on a large variety of factors such as food and drink volume and composition, vitamin and mineral balances, stress, hydration, liver and pancreas function, insulin sensitivity, exercise, mental health, and sleep.
Carbohydrates you eat, with the exception of indigestible forms like most fibers, eventually become glucose in your blood. Assuming your metabolism is functioning normally, if the switch is on you will store fat. If the switch is off, you will burn fat.
Therefore, all things being equal, “diets” are just ways of hacking your body into a sufficiently low-glycemic state to trigger the release of a variety of hormones that, in turn, result in a net loss of fat from long-term storage.
That pretty much sums it up.
If you want to lose weight from fat cells, those cells need to store fewer calories than they release. What most people do not understand, however, is that this is not as simple as “calories consumed” vs. “calories burned”; your body responds very differently to 200 calories from a cookie, for example, verses 200 calories from broccoli.
Furthermore, as long as protein-intake is reasonably high enough, your body will not burn a significant amount of muscle protein (i.e. you won’t lose muscle mass, but you will lose body fat).
If you’re curious to read more about the details, I spend a fair amount of time below introducing the science of how carbs, fats, proteins, fibers, alcohol, caffeine, vitamins, minerals, water, gut microbiota, lipoproteins, cholesterol, sleep, exercise, mental health, etc… contribute to overall fat metabolism.
What is Fat?
“Fat”, depending on the context, can mean different things (e.g. specific molecules, cells, tissue/food, and/or a physical body state). On a cellular level, there are a bunch of different types of fat cells and fat tissue. What most people are referring to when they are talking about the biology of “fat” is white fat cells, especially those located just under the skin (i.e. subcutaneous fat).
Below is a simple illustration from wikipedia that gives us a decent idea of the tissue and cells we’re talking about:
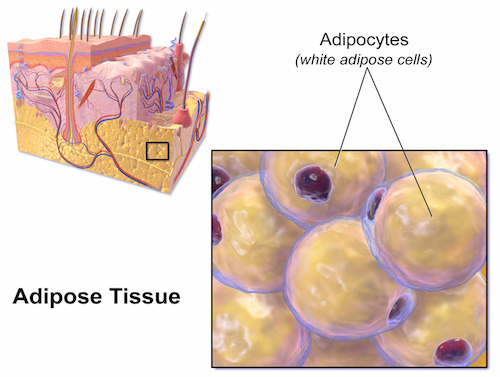
Those large white blobs (termed “lipid droplets”) in the white fat cells are what house our triglycerides (TAGs…get used to this acronym, I’m going to use it a lot). The lipid droplets are what grow and shrink as TAGs come and go. Chemically speaking, TAGs come in different varieties, but are always made up of a glycerol molecule plus three fat molecules, resulting in a structure that looks essentially like this:
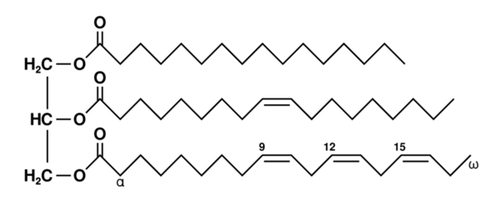
The alpha (α) “first”, omega (ω) “last”, and numbers on the bottom part there are labels (from a chemist’s perspective) for specific carbon atoms. On the other hand, biologists, to make our lives easier (I’m joking), count from the other direction. You may have heard of Omega-3 Fatty Acids, which means the third carbon from the right has a double bond. Indeed, the keen observer will see that the bottom molecule in the figure above is an Omega-3. And yes, FYI, a “fatty acid” are those long squiggly things. So when you say the word “fat” to a biochemist, these are the molecules that come to mind.
As a final point of technical background here, let’s clarify “saturated” versus “unsaturated” fat. This terminology has to do with the “saturation” of hydrogen atoms around the carbon atoms. Simply put, unsaturated fat has double bonds between one or more of of its carbon atoms (i.e. the double line things) and saturated fat are those that don’t.
You’ve probably heard scary and opinionated things about saturated vs. unsaturated fat, and by all means, do what your doctor tells you. But for some peace of mind, know that your body needs both to function properly.
How do fat cells grow?
So, given the background above, the specific question we’re curious about is what causes TAGs to accumulate in lipid droplets within white fat cells?
As you can imagine, the current answer (subject to change) is quite complex. I’m going to start the answer by categorizing the types of substances we consume into general buckets (there are, of course, more… but this provides sufficient coverage for our discussion here and helps us think carefully about what we eat and drink).
- Carbs — At the end of the day, starches and sugars we eat (from bread, pasta, corn, potatoes, desserts, etc…) are broken down in your digestive system into monosaccharides. The two main monosaccharides we’ll consider in this article are glucose and fructose, since they are overwhelmingly the most common (and therefore the most important regarding fat metabolism).
- Fiber — The various forms of carbohydrates we eat that aren’t digested are commonly called fiber. Fibers come in water soluble and insoluble forms and facilitate digestion of everything else we consume.
- Fat — These are the oily molecules that contain saturated and/or unsaturated carbon chains as mentioned above. They come in the form of TAGs, various other combinations of fat molecules, and as “free fatty acids” from a gazillion different kinds of oils and animal fats. (As a side note, Trans fats, which are common in processed foods, are a type of unsaturated fat that is altered to a form that is not usually found in nature. Here is more specific information about why the FDA is concerned about them)
- Protein — There are 22 standard building blocks (“amino acids”) that make up all proteins in the human body. Nine of these are not able to be produced by our bodies, so we need to ingest them (hence, they are termed “Essential Amino Acids”).
- Caffeine — This merits a bucket of its own since we consume so much of it. There’s a reason why the classic “diet pill” has large amounts of caffeine in it.
- Alcohol — This also merits its own bucket, since we love to drink. Alcohol is a known “toxin” and has important, though debatable, effects on fat metabolism.
- Vitamins & Minerals — Many vitamins and minerals are important in direct (and indirect) ways for our discussion. As we’ll talk more about below, it’s a good idea to take supplements, under the guidance of your doctor, if you restrict common foods (e.g. dairy, gluten, etc…) from your diet.
- Water — Last but not least, if you drink too little or too much water it can throw your whole system off, as every chemical reaction in our bodies involves water in one way or another.
Now, given these general buckets, let’s talk about how each one relates to TAGs filling up our fat cells.
Glucose Metabolism
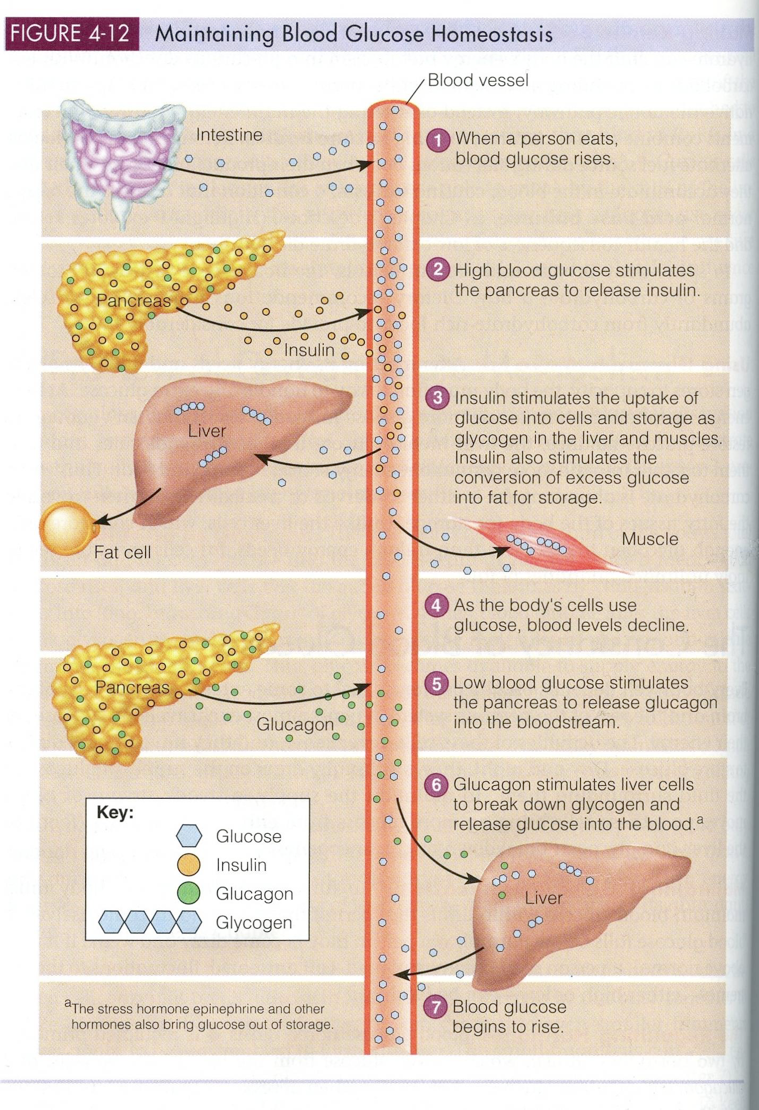
First and foremost, out of all the buckets, it’s important to note that glucose is by far the major player here. While on a normal “well-balanced” diet, the concentration of glucose over time in your blood is the key upstream factor to consider in the metabolism (both build-up and break-down) of fat.
When your blood has high concentration of glucose for a sufficient period of time, your pancreas kicks insulin into gear, which tells your cells to take in glucose, put it in a temp storage (like RAM in your computer) called glycogen, and put everything else into long-term storage inside your fat cells.
On the other hand, when your blood has a low concentration of glucose for a sufficient period of time, this process is reversed. Your pancreas releases a protein called glucagon, glycogen is depleted, a bunch of other hormones (epinephrine, cortisol, testosterone, etc..) are introduced into your system, and TAGs are thereby pulled from your fat cells and converted into Acetyl Co-A, which is the key precursor for the process your body uses to generate “energy” (i.e. ATP) for your cells.
So, as it relates to our digestion here, a key process to consider is the adsorption of glucose into (and across) your intestinal wall. It’s a relatively short story. This is why when you eat/drink sugary stuff it goes quickly into your blood. These blue and green transporters (yes, it’s active transport, not passive, which means it takes energy) are efficient at getting the job done:
It’s important to note that the rate of getting free glucose into your bloodstream is quite high when you have, surprise surprise, free glucose in your lumen (intestinal tube). Once glucose gets into your blood, then insulin does its job. Here’s a simple graphic that describes the basic process:
But before we get too far ahead of ourselves, let’s talk a bit about what form glucose takes as we consume food and drink. Most of our glucose is packaged in starches (breads, pasta, corn, potatoes, and such), but we also get a fair amount via common table sugar, too (i.e. sucrose). This chart shows the basic breakdown pathways of starch, sucrose, and lactose into glucose:
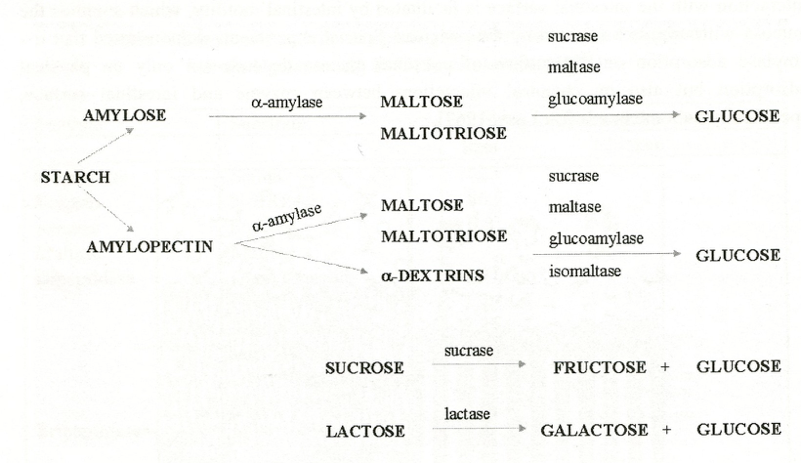
As an important side note, High-Fructose Corn Syrup (HFCS, which is in everything these days) is our food industry’s way to mimic table sugar (sucrose) for a lower price. Most HFCS in soft drinks is 55% fructose and 42% glucose, and HFCS in pretty much everything else is 42% fructose and 53% glucose. The rest of the percentage, for those doing the math, is maltose or maltotriose — that is, 2 or 3 glucose molecules bound together, respectively.
From a biochemistry standpoint, know that HFCS is essentially just fructose and glucose mixed together. It takes a bit more “work” for our body to breakdown table sugar (i.e. via sucrase, as noted above), which means glucose from HFCS goes into our blood “faster”, depending on what you eat with it. Again, this consideration (i.e. the speed in which glucose gets into our blood and its concentration there) is the most important thing to talk about when it comes to regulating fat storage in our body.
Fructose Metabolism
Ok, so we know that glucose gets into our blood quickly and is used by all cells, stored temporarily in glycogen, and stored long-term in fat cells. But what about fructose?
Structurally, here is the exact difference between glucose and fructose:
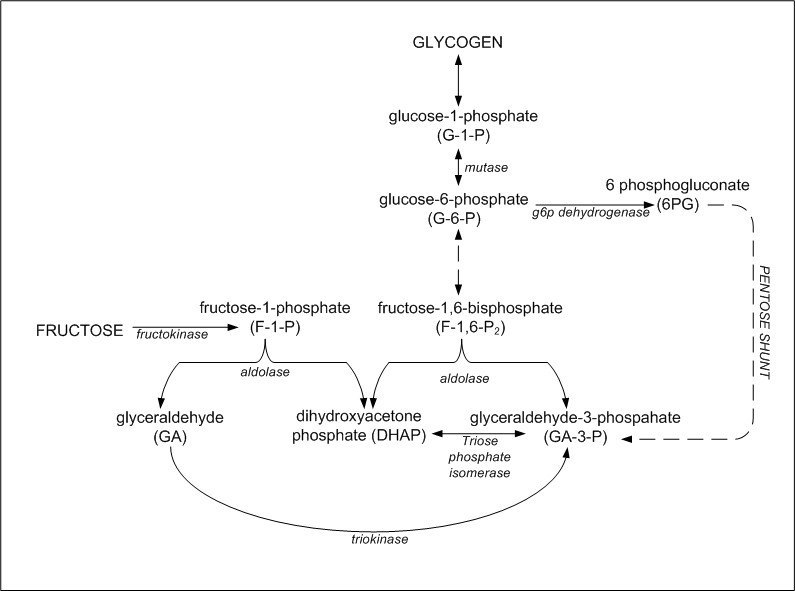
As you can see, both have six carbons, but the fructose carbon ring is smaller (the other carbon is hanging off as an additional CH2OH group). But why does this matter? Well, for one, fructose tastes sweeter to us (which is nice, I suppose). Second, fructose is absorbed into our blood via a slightly different route than glucose, and is relatively slower to do so unless ratios of glucose to fructose are similar. Third, once in your blood, fructose can only be processed by your liver, where — when introduced in reasonably low concentrations — it is converted to glucose and mainly stored in glycogen:
However, in higher concentrations, and especially when there is plenty of glucose around, fructose can do unhelpful things, including a more direct route to storing TAGs in our fat cells and a propensity toward non-alcoholic fatty liver disease (NAFLD):
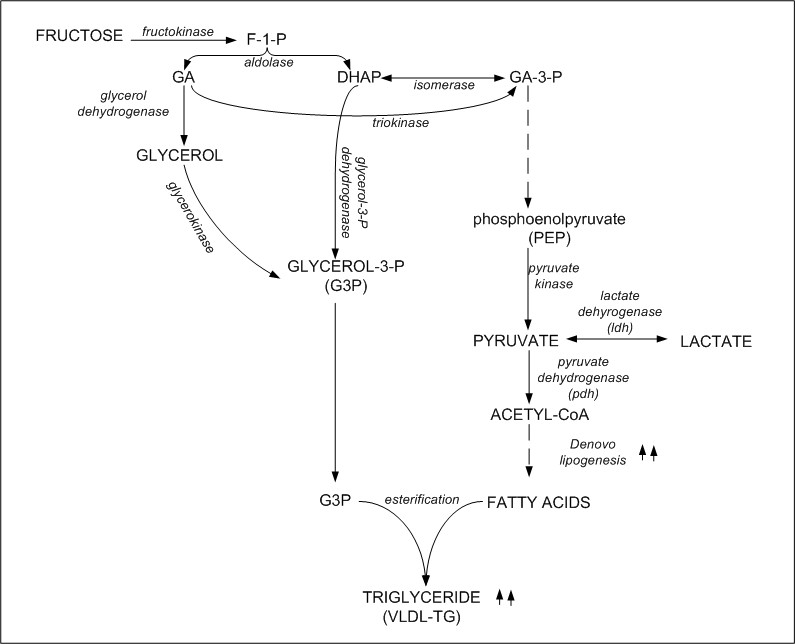
Fructose does not stimulate insulin like glucose does, so in small amounts fructose participates relatively harmlessly with our normal energy storage and supply. But, indeed, part of the reason why soft drinks with HFCS are so “bad for us” is because it’s easy for us to drink too much, which thereby sends a significant percentage of it into our fat cells (especially around the liver).
Fiber
Now that we know the basics of TAG production and storage from glucose and fructose, we can better understand why limiting the rate of adsorption of these molecules into our blood is important. This is — in part — where fiber comes in, and is a component of why the recent craze around eating “whole foods” is significant. Unprocessed foods generally contain more fiber (as well as more vitamins and minerals, which are often leached out during processing).
The below chart nicely sums up a ton of information about why fiber is important for overall fat metabolism.
It has been well documented that increased fiber in the diet reduces the concentration of glucose in the blood. The mechanisms behind this are not completely known, however, but it is likely because of a binding effect that prevents the degradation of carbs into free glucose.
Fat
If you’ve ever gone on a low-carb diet while still eating a decent amount (if not more) fat, you’ve probably been surprised that you actually lost weight. What’s up with that? Doesn’t eating fat make you fat?
Well, to answer this, let’s go ahead and follow the same process we did above with glucose and fructose.
First, when you ingest fat, your digestive system breaks it down to its component parts, i.e. free fatty acids and monoglycerides. And, as you can guess, the rate of this degradation depends on what else you are eating (e.g. fiber). Once the molecules are freed up, they are adsorbed via a completely different mechanism than glucose and fructose. Here is a great summary:
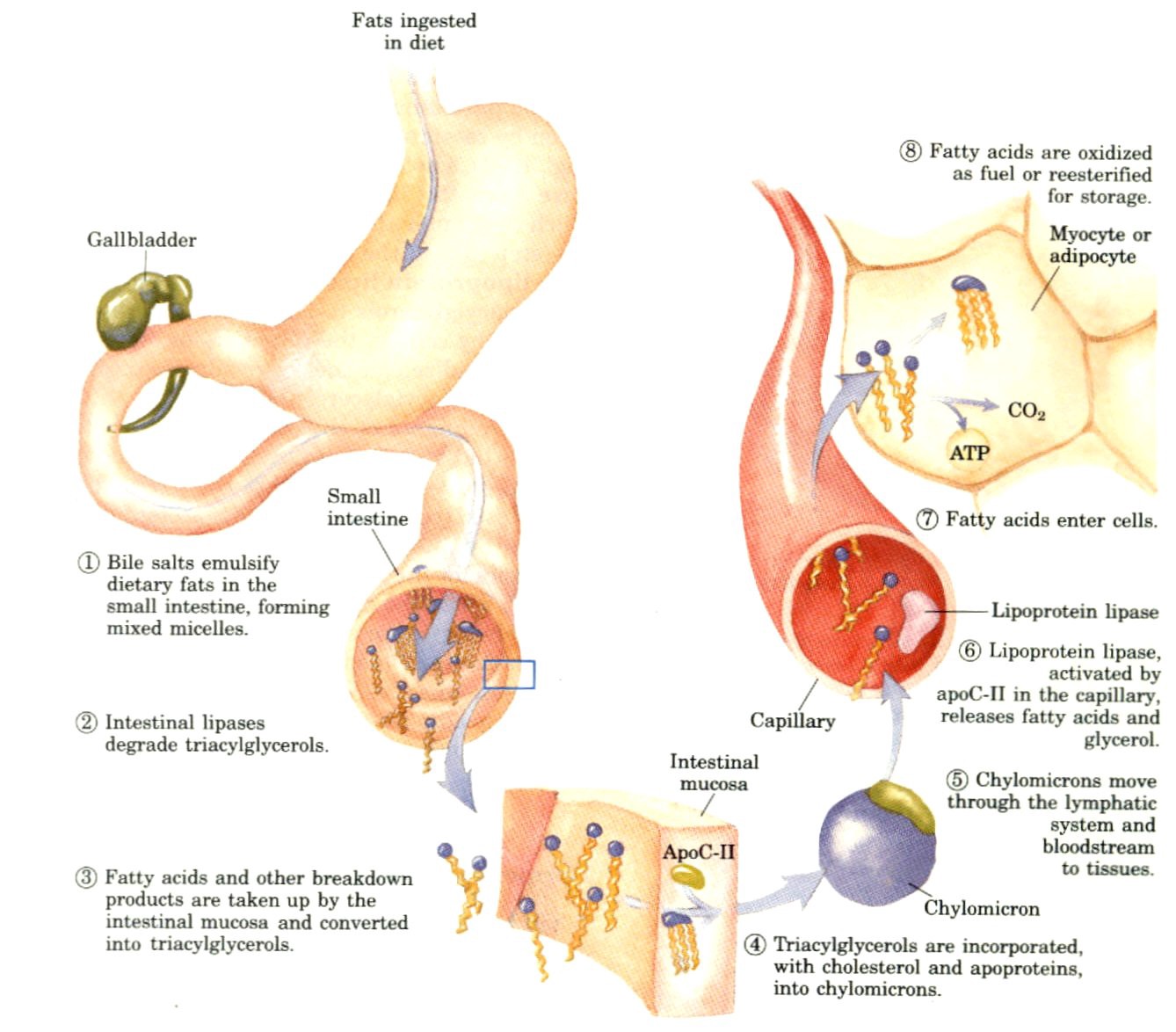
Getting more specific on that last step there, here is how fatty acids are ultimately turned into energy:
Lipoproteins and Cholesterol
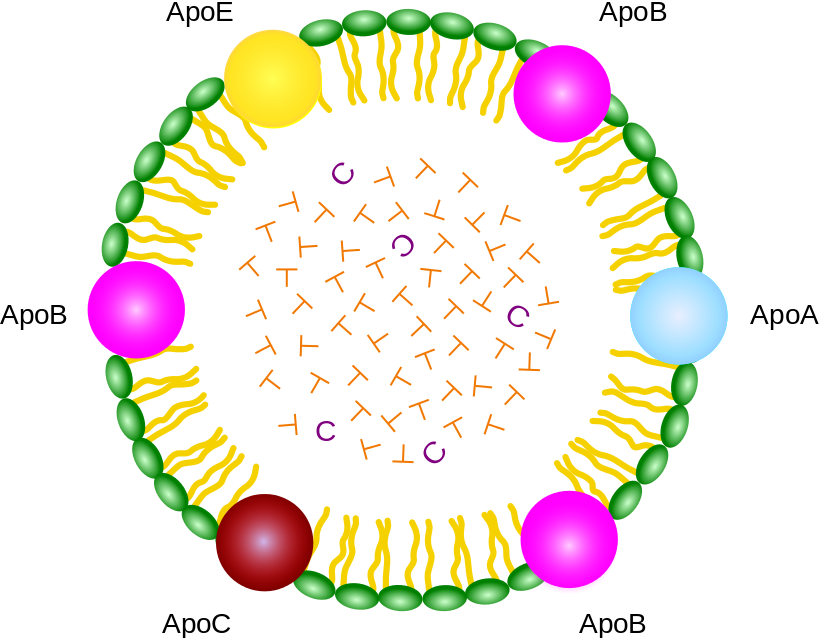
In addition to the mechanisms it takes to get energy out of fat molecules, it’s important to note (albeit somewhat tangentially) what else our body does with fat. Here is the basic structure of a Lipoprotein, which our cells produce to move fat, cholesterol, and other lipids around the body (T = TAGs, C = Cholesterol):
You may have heard of “HDL” and “LDL” when visiting the doctor and reviewing your blood work. There are actually five different types of lipoproteins that vary in size and density (H = “High”, I = ‘Intermediate’, L = “Low”, VL = “Very Low”, D = “Density”, L = “Lipoprotein”) :
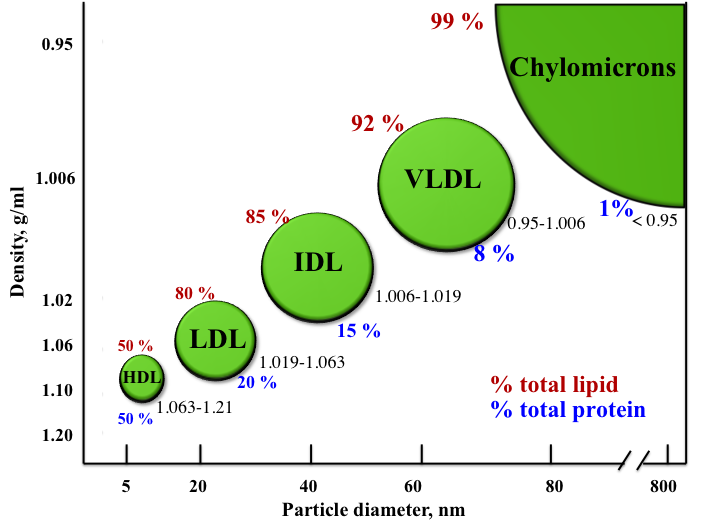
From large to small,
- Chylomicrons carry TAGs and cholesterol from the intestines to the liver, muscles, and fat cells.
- VLDLs carry new TAGs (with cholesterol) from the liver to mainly fat cells.
- IDLs are general transporters that are essentially VLDLs with the TAGs removed.
- LDLs are also general transporters that carry mainly cholesterol, fat-soluble vitamins, TAGs, and phospholipids out from the liver to cells around the body.
- HDLs mainly carry TAGs and cholesterol back to the liver.
Cholesterol, FYI, is critical for our health since it’s a key ingredient in our cell membranes, and it’s the key precursor for vitamin D, bile salts, and a bunch of critical hormones. Our bodies produce all the cholesterol it needs (from, yes, our friend Acetyl Co-A), and — contrary to popular opinion — consumed cholesterol doesn’t really effect our lipoprotein profiles or risk for heart disease.
The reason why our discussion of lipoproteins is important for fat metabolism is because HDLs are needed to properly respond to the call to get energy out of our fat cells. It’s also better for us to simply be informed about how this all works, to be less afraid of ingesting fat.
Protein
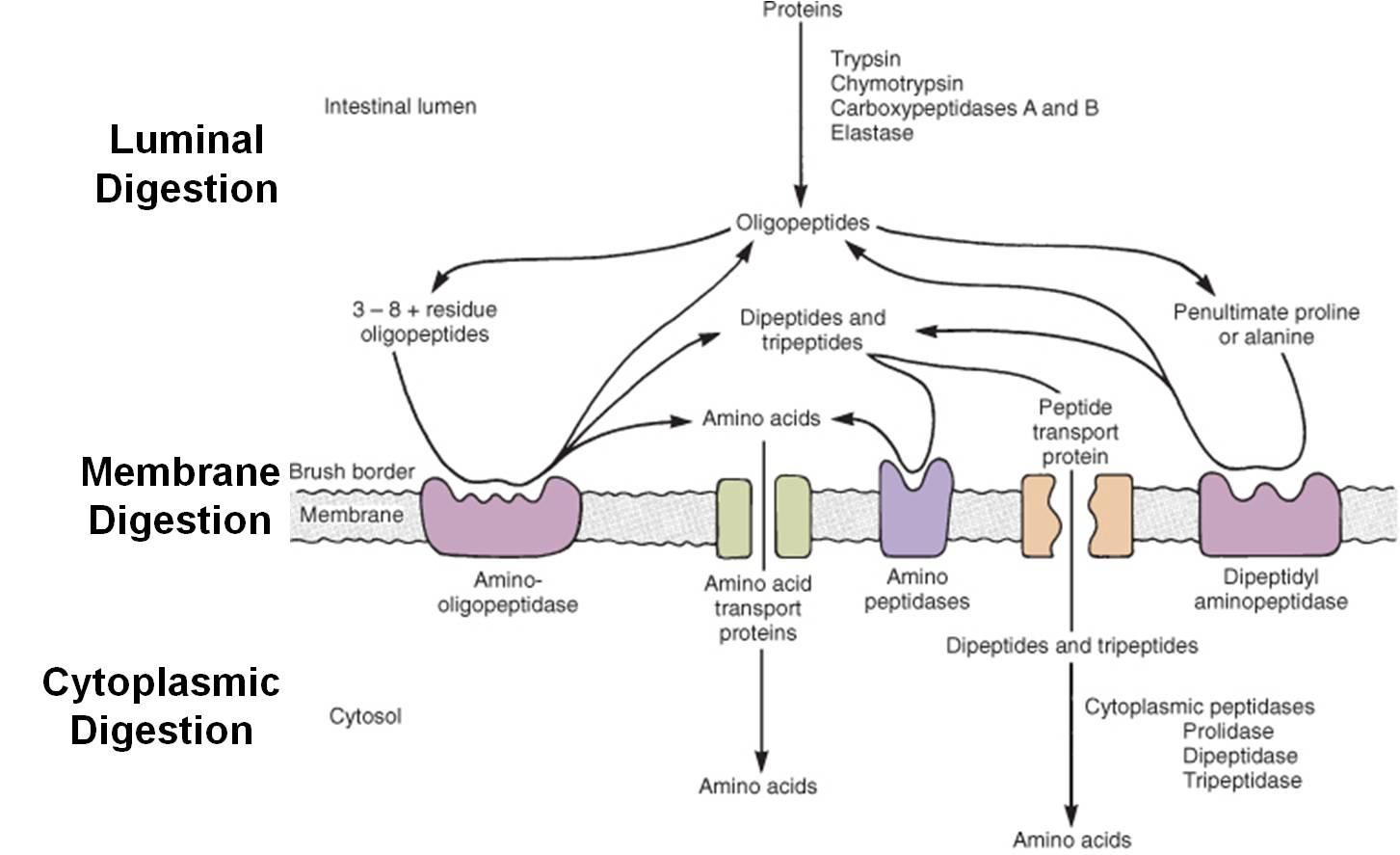
Can protein make you fat? The short answer is yes, but not efficiently. When you eat protein, it gets broken down into “peptides” (i.e. chains of amino acids) and absorbed into the blood via mechanisms like this:
Free amino acids in the blood can then be used for energy, including getting converted into pyruvate and acetyl Co-A:
And as you can see, this is mainly for the purpose of getting energy out of our proteins, but it is possible that in excess, the Acetyl-CoA can get converted into fat (per the mechanisms described above).
At the end of the day, however, amino acids are “best” used for actually building and maintaining proteins in our body (including those in muscle tissue).
Caffeine
As we consume caffeine, an energy spike kicks in and — as we consume even more — most people get jittery and less coordinated. The basic mechanism here is to block your nervous system from getting drowsy and to increase hormones such as epinephrine (a.k.a. adrenaline). Caffeine itself is not the energy, despite what marketing from “energy drink” companies will tell you.
As it relates to fat metabolism, caffeine has been shown to promote TAG release from fat cells. While it’s not clear exactly how this happens, it’s thought to be a combination of the properties of caffeine itself along with the effects of epinephrine (i.e. calling for energy release).
Thus, diet pills are often packed with caffeine and, for some people, actually help the weight loss process. For others, the negative effects of caffeine (e.g. lack of good sleep) actually counteract the process and lead to a net weight gain.
So, in short, be careful with caffeine. I’ll leave it at that. Again, always consult with your doctor on these issues if you have questions and/or are considering changing your diet.
Alcohol
When you consume alcohol, you are consuming “calories”, but the relationship to fat gain/loss is highly debatable.
Looking at the basic science, alcohol can indeed be turned into Acetyl-CoA via:
…which in turn, similar to what we described downstream from fructose and protein above, can lead to fat production and storage (especially around the liver) with sufficient biochemical “pressure” (e.g. when blood glucose levels are high).
Another proposed effect of alcohol on weight control is blocking the oxidation of lipids (i.e. the process of getting energy from fat). One such study in the New England Journal of Medicine showed that alcohol can lead to weight gain if the body already has enough energy in place, saying:
the ingestion of ethanol as additional energy above nutritional requirements is a risk factor for obesity, because it decreases lipid oxidation and therefore favors lipid storage.
Finally, and perhaps more obviously, when you drink your judgement is impaired. Thus, you’re less inclined to actually “listen to your brain” that’s telling you to stop eating.
Vitamins and Minerals
Vitamins (A, Bs, C, D, E, K) and minerals (calcium, magnesium, zinc, iron, etc…) are key components and regulators of many of the processes described above. Notable examples are B1, B2, and B5, which are all involved in the various stages of deriving energy from fat, proteins, and carbohydrates. Furthermore, Iron, Niacin, and B6 help metabolise L-carnitine, which is essential for the transport of fatty acid components to energy-producing areas of cells.
The list of similar examples is extensive, but what is key for our discussion here is that if you are deficient in any vitamin and/or mineral, it can mess up all your other efforts. For example, being low in Vitamin D or Calcium can affect your ability to stop eating, and being low in magnesium can seriously mess with your insulin sensitivity.
Therefore, it’s a good idea to have your blood checked on a regular basis to see if you have any vitamin or mineral problems. Getting to a healthy baseline here is, obviously, an important component to overall health.
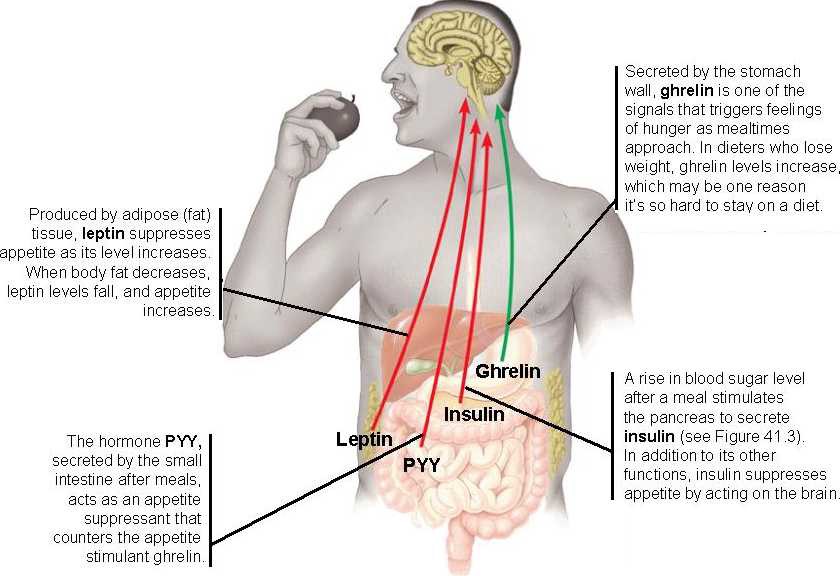
Hunger and Satiety (i.e. Feeling Full)
In the areas of appetite control, yet again we run into a “highly complex” set of overlapping systems. The basic elements are:
- Physical volume — your stomach has stretch sensors that tell your brain when to eat and when you’ve had enough. This is, in part, why eating low-density, high-volume foods (like leafy greens) are important for satiety.
- Fat/Carb/Protein ratios — everyone is slightly different, and it depends on what you’ve been eating the past couple of days, but in general your digestive system wants to receive a decent balance of these basic macronutrients.
- Vitamin & mineral diversity — we’ll often crave particular foods if we’re lacking vitamins and/or minerals (e.g. craving chocolate when low in magnesium, craving red meat when low in iron, etc…)
- Mental health — depression, anxiety, and other mental health disorders often have a significant impact on hunger and satiety (one way or another).
- Sleep — not getting enough can be problematic (we’ll talk a bit more about this in the next section).
- Dehydration — not drinking enough is also cause for concern, and drinking more water (as our intuition always suspects) helps significantly with satiety.
Underneath these factors are four important hormones that regulate appetite:
Sleep
Sleep is extremely important regarding obesity in children and in adults. This topic merits an entire series of articles (and books!) on its own, so I’ll refer you first to Matthew Walker’s book Why We Sleep and his podcasts/AMAs with Peter Attia.
Long-story short, a lack of length, diversity, and “quality” of the various stages of sleep will have dramatic effects on a large number of biological systems, hormone levels, and cognitive functions related to energy metabolism. Focusing on improving all aspects of your sleep is essential to healthy fat loss.
Gut Microbiota
Another area of fat metabolism research that is gaining popularity concerns the population of bacteria inside our intestines. Early research shows that its relationship to dietary fiber, the absorption of carbohydrates and fat, and effects on appetite are more significant than previously thought.
One of the concerns of taking strong antibiotics, for example, is that it can throw off your gut microbiota and possibly lead to weight gain. On the flip side, some strains of probiotics may actually lead to weight gain as well.
Thus, how your gut microbiota adjusts to your diet over time, and how food, drink, and medications may affect this composition will be, as many suspect, a significant area of research in the near future.
So….should I still count calories?
If you’ve read this far, you’ve hopefully realized that not all “calories” have the same effect on fat metabolism, and that counting calories can be an overly simplistic way to think about it. Here is a decent summary graphic of the basic pathways for proteins, carbs, and fat:
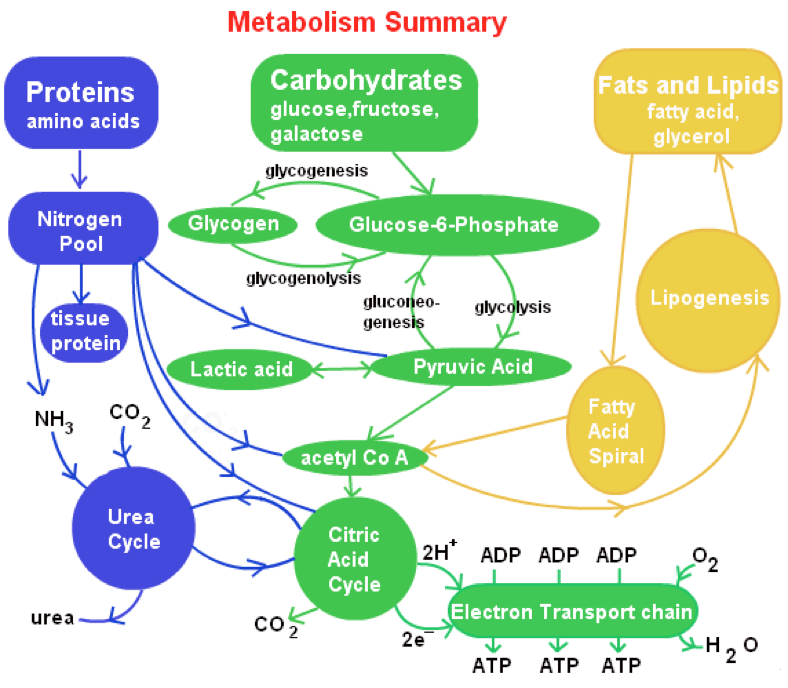
In other words, your body will get energy one way or another, but one of the best ways to effectively burn energy from fat-cell TAGs is to keep your carb consumption low. By a long shot (as anyone who has ever gone on a low-carb diets knows), our body strongly prefers to use the green route above for energy. If you tweak your diet to make your body use mostly the yellow route for energy, it — by definition — facilitates overall fat burning.
What about exercise?
Everyone should exercise daily, mixing up high-intensity and low-intensity cardio, stability/flexibility training, and lifting weights. There really isn’t any debate on this. Exercise burns energy stored in glycogen and fat, which helps your body regulate blood-sugar levels and overall energy metabolism.
However, unless you are an extreme athlete — or go through periods of extreme exercise — contrary to popular opinion, cardiovascular exercise rarely has a significant impact on the overall quantity of TAGs in your fat cells. While indeed you expend energy and burn through glycogen and fat when you workout for long enough — your body adjusts for this via increased hunger and consumption of carbs, fats, proteins, etc…
As you may have heard, building muscle does, indeed, raise your basal metabolic rate (so it’s a good idea to lift weights!). But again, your body adjusts to this new rate by compelling you to eat more. In fact, in order to gain muscle you need to be in energy-positive situation and let insulin do its work of bringing in energy and amino acids in for “muscle building.”
So, with regard to fat metabolism, this is a short section of the article. Everyone should exercise daily for overall muscular, cardiovascular, and mental health.
How do we shrink fat cells, then?
In order for our bodies to start pulling TAGs out of lipid droplets, the appropriate signals need to be sent to receptors on the surface of fat cells. When glucose resources are low, this activates a wide variety of hormones to help get the job done, including (to varying degrees and roles) epinephrine, norepinephrine, corticotropin (ATCH), thyroid stimulating hormone (TSH), cortisol, ghrelin, testosterone, human growth hormone (HGH), adiponectin, cholecystokinin (CCK), glucagon, and leptin. Here is a sample of the receptors that have been discovered on fat cells:
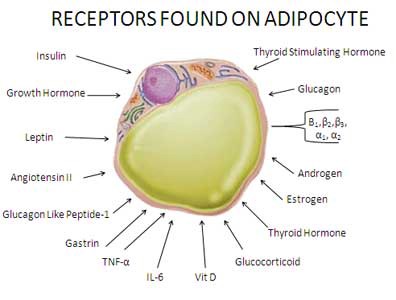
Not all are involved in telling adipocytes to release TAGs, however (though many, indeed, are, giving you an idea of the complexity here).
Below is the basic process by which leptin, as an example, stimulates the brain to signal the release of “fight or flight” (sympathetic) hormones that kick fat burning into gear.
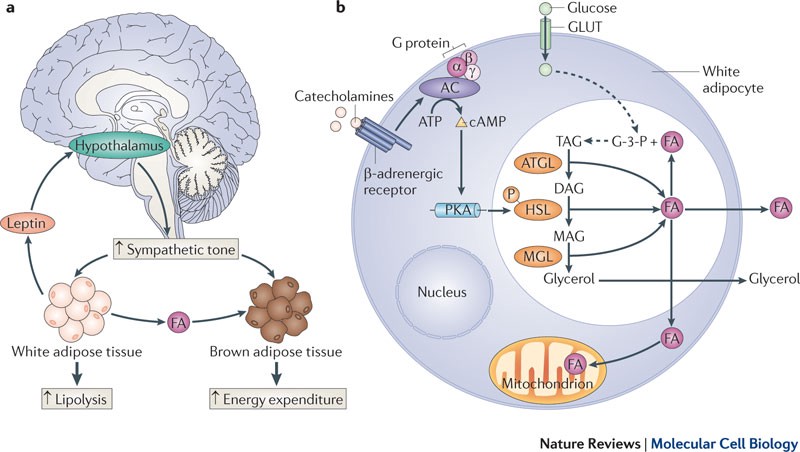
And it’s not just catecholamines (epinephrine and norepinephrine) that are involved, many of the hormones mentioned above also activate PKA (Protein Kinase A) in fat cells and work with ATGL, HSL, and MGL to break down TAGs and kick out fatty acids (FA) and glycerol.
So, as you can see, to lose weight all you need to do is keep glucose levels down, make sure that these hormones are triggered effectively, and don’t eat more calories than you burn, right?
Easier said than done
Everyone has a different “metabolism” (i.e. the rates and efficiencies of the metabolic pathways and biochemistry described above), and these factors always change as we get older. In other words, genetic and environmental factors will make it virtually impossible for some people to have a low body mass index (and vice versa), and most Americans are destined for an increasing BMI until the age of 60 or so.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This chart is especially disturbing since the Center for Disease Control indicates that a BMI of 25 or above is “overweight.” Uh oh. If you have a relatively large amount of muscle mass it will throw your BMI calculations off, but it’s an important metric for the overall population.
Now, there is the other end of the spectrum, as all of us suspect in the back of our heads. There are risks to low BMIs. One study found that “adults who are underweight — with a BMI under 18.5 or less — have a 1.8 times higher risk of dying than those with a “normal” BMI of 18.5 to 24.9.” But, to put that in perspective, if you are 5’5” you’d have to weigh less than 111 pounds, and if you are 6’0” you’d have to weigh less than 137 pounds.
Ummmm…so how can I lose fat?
To actually get into a “fat-burning” state, the simplest explanation is to keep your blood-sugar level low for as long as possible and ensure nothing is getting in the way of your metabolism (e.g. vitamin/mineral imbalances, stress, lack of sleep, etc…). Obviously, people lose weight on diets all the time; and at the end of the day — biochemically speaking — this is how it always happens.
Whether you pick a low-fat or a low-carb diet, it’s mostly a mental game. Maybe eating a small amount of carbs 4–5 times a day (along with a bit of fat and protein) makes you feel better and you can actually keep your overall glucose and insulin levels low. Or, maybe you prefer to essentially cut the carbs and keep eating reasonable amounts of fat and protein. You need to experiment yourself — and consult with your doctor — to figure out what works for your unique metabolism.
But, that being said, knowing “the science” behind all this can help us think through a few things:
- Glucose in the blood spikes insulin, and if your glycogen stores are full and your cells aren’t directly needing energy, glucose will get converted to acetyl Co-A, built into TAGs, and shoved into your fat cells.
- On the flip side, a low level of glucose is what triggers glucagon to get energy from glycogen, and it’s what triggers hormones such as epinephrine, norepinephrine, cortisol, ghrelin, testosterone, human growth hormone, etc… to pull TAGs out of fat cells for energy and to compel your body to eat.
- A great way to keep your glucose levels in check is to eat food/drink combinations that slowly move glucose into your blood. This is where “whole foods” and fibers come into play, which also help with vitamins and mineral diversity. There are various “indexes” (e.g. glycemic index, insulin index, satiety index, etc…) that can help you identify food/drink to try experimenting with yourself, but these indexes are not an exact science because various combinations of foods you eat together can change things up.
- The key game to play is with appetite and mental sanity. When your glucose levels are low, your body hates you until you adjust to a ketoic state. For low-carb diets, hours 48 through 96 (ish) are the worst as you transition, and then you start feeling better. The long term effects of staying in diet-induced ketosis are debatable, though practically speaking our culture (in America, at least) does not facilitate low carb diets, so few people make it longer than 7–9 months anyway (and, BTW, that time frame is generally safe). Those that do go that long, however, usually enjoy about a 20–40+ lbs weight loss, but rapidly gain it back because controlling weight with more carbs in a diet is really, really hard.
- Alcohol combined with a bunch of carbs will help you gain weight, but if you keep glucose levels low, your body will use it for energy and avoid converting it into TAGs for long-term storage.
- Caffeine, in moderation, can help boost your epinephrine levels to promote fat burning. Too much can throw you off, however, and cause you to consume more glucose to balance things out.
- Do what your doctor tells you (and find a doctor who isn’t afraid of salt and healthy fats).
- Get regular physicals and specific blood work done that checks for mineral/vitamin imbalances.
- Understand that exercise is important for muscular, cardiovascular, and mental health (and sleep), and you should do it daily, but it’s effect on fat loss is minimal unless you change your diet.
In conclusion, the best game to play here is how to hack the mental process of staying reasonably “healthy” (however you and your doctor define that) while not freaking out about having a few TAGs in your fat cells. Knowing all the science above should help each of us, in concert with our health care providers, put together a customized plan for long-term health.
Author’s note: I’d love to hear from anyone with suggestions on how to improve this article. I’m currently researching how various food combinations affect blood-glucose concentration, and how its specific rate-of-change and absolute value over time affects fat metabolism. Subscribe to my newsletter and I’ll let you know when I get new content up (I write mostly about startup/tech stuff, but occasionally I’ll write articles on topics like this). Let’s keep the conversation going. Thanks!